Contents
March
16, 2019
Rana R. McKay, MD, is a
board-certified medical oncologist who specializes in treating people with
genitourinary (urologic) cancers, including bladder cancer, kidney cancer,
prostate cancer and testicular cancer. Dr. McKay is part of the urologic cancer
unit at UC San Diego Health’s Moores Cancer Center, where she works alongside a
multidisciplinary team to provide patients with highly specialized care. Dr.
McKay will be discussing the Evolving Management of Patients
with Metastatic Cancer & will highlight upcoming
clinical trials of interest.
February
16, 2019 Member Panel
Summary by Bill Lewis
1. Tim D’Andrea is 60 years
old, and an engineer who went into technical sales. “My Journey.”
He is currently in remission, after 31 sessions of proton therapy and 18
ongoing months of Lupron. His PSA is
0.24 and still dropping.
He
was diagnosed in early 2018. MRI-guided
biopsy found one core of Gleason 4+5, and a subsequent Ultrasound-guided biopsy
found Gleason 3+3 and 4+3 in one side of the prostate.
During
the previous two years, his PSA was in the range of 6 to 7. His FreePSA was 5%, suggesting a 49% chance
of prostate cancer. The PSA4K test gave
77% odds of high-risk prostate cancer.
His urologist pushed him to accept a random biopsy (not having the
MRI-guided option there at Sharp Rees-Stealy), and had no knowledge of any
support groups. He declined the biopsy,
joined the IPCSG (“best thing I ever did”), and dove into research on the
disease and his options.
He
tried a naturopathic approach, including lifestyle (diet and exercise),
supplements (apple cider vinegar, flaxseed oil, ginger root, baking
soda/molasses, pomegranate extract, curcumin, Maitake, etc.) and 100-g doses of
IV vitamin C. He also cut down on
work-related stress – his company approved a four-day workweek for him. A second naturopath tried two antibiotics to
rule out infection, checked with Color Doppler ultrasound (“normal” result),
and gave many more (unpleasant) supplements.
His PSA remained steady for about a year.
But
then, his PSA rose to 9.5 in October 2017, so he put his IPCSG knowledge and
network into high gear. The MRI guided
biopsy mentioned above was done in early 2018, with only four cores. It was essentially painless, and gave hope
for a focal treatment. But he had a
second biopsy with 12 cores (and no anaesthesia – ouch!), which found more
widespread cancer within the prostate, eliminating his hope of a focal
treatment. In retrospect, he feels that
more cores should have been taken in the MRI-guided session.
Dr.
Scholz at Prostate Oncology Specialists recommended Radiation + ADT. Tim changed his medical network to UCSD,
where Dr. Mundt recommended proton therapy, not X-rays (That’s a sign of a
great doctor – he recommended a treatment other than his in-house
capability!). So he went to California
Protons, and was treated as noted above by Drs. Einck and Rossi. Last September, he was declared by Dr. Einck
(also of UCSD) to be in remission, and told that he needs no biopsy now – just
ongoing PSA testing.
Overall,
he’s very pleased with his outcome, with IPCSG, and with his wife’s full
participation (appointments, IPCSG meetings and research help). His regrets are having delayed the initial
biopsy, and not having more tissue samples in the first biopsy.
2. Elliot Shev
and his wife, Dr. Wendi Maurer (clinical psychologist in grief and
loss), with “Our Prostate Cancer Journey.”
Elliot is 71 and managing a facility in Tijuana for a large Japanese
company. Current status: PSA = 1.7, feeling great, with all functions
working fine.
After
5 years with his annual PSA hovering around 3.0, it rose to 4.7 by December
2017. After two weeks of antibiotics (to
see if it was an infection), the PSA was 5.5, so they needed to make a
decision. They chose immediate action,
and went to see a urologist. This led to
a biopsy (not pleasant!) and Gleason score of 4+3, with Stage = T2b (one side
of prostate diseased). He was given a
bone scan and a “high contrast abdominal MRI.”
They
were referred to a surgeon and radiologist.
They recorded every conversation, and had them transcribed. They talked to family members (some are
experts in medicine) and “everyone” they knew, despite this aggressive
inquiring leading to occasional embarrassing moments (“What’s your PSA?”). Surprisingly, very many of them “had a
story,” and they always made notes. They
found that two friends had had HIFU (high intensity focused ultrasound)
treatment.
HIFU
is a “non-invasive” procedure which uses sound waves to image and destroy
prostate cancers. Using real-time
imaging, precise, focused ultrasound energy is delivered to the diseased cells
of the prostate. Ideal candidates (per
Stanford Healthcare) are men who hope to preserve continence and sexual
function, currently have satisfactory sexual function, have cancer visible in
MRI and confined to the prostate, and have a PSA below 20. Some references: “A Multicentre Study of 5-year Outcomes
Following Focal Therapy in Treating Clinically Significant Nonmetastatic
Prostate Cancer,” in europeanurology.com.
FDA approval -- Medscape.com/viewarticle/853120. Doctors: Dr. Robert Pugach, Los Alamitos, CA,
HIFUprostateservices.com and Dr. Steven Scionti, Sarasota, FL,
sciontiprostatecenter.com. Much more
info is available from Elliot by email on request (via the IPCSG).
Only
the half of Elliot’s prostate which contained the tumors was treated, so he still
has half of his prostate. Treatment took
about 2.5 hours under total anesthesia, with 4 hours total at the clinic. His PSA dropped in 90 days from 5.5 to 1.7. He will be retested every 90 days for the
first year, then get an MRI and a checkup with Dr. Scionti.
Lessons
learned: Be your own advocate and case
manager! Get an MRI prior to a biopsy,
which should then be targeted. Talk to
everyone. Don’t turn away loving
support. Be patient with yourself and
others. Doctors mean well, but they
don’t know everything, and they are good salesmen for their specialty. Always, be your own advocate and case
manager.
3. John Tassi is 63 years old, in satellite
communications, and a 9-year survivor in remission. “What to Do if Your Prostate Cancer Doesn’t Return.
“ In retrospect, his gradually rising
PSA in his 40’s, reaching 3.5 at age 49, was an indication of prostate cancer,
though his DRE (rectal exam) was still normal.
The next year, he was incorrectly diagnosed with BPH (enlarged
prostate). Two years later, in 2007, his
PSA reached 19, still with a normal DRE.
His doctor said, “You are too young for prostate cancer.” In December 2007, a biopsy revealed Gleason
3+3 on the right side and 3+4 on the left side.
He chose Robotic-assisted Radical Prostatectomy, which was done in
February 2008. Pathology of the removed
prostate showed both sides had Gleason = 4+5, and that the margins were
positive (Bad!). His PSA rose, doubling
between August and October, so in December he started 37 sessions of IMRT (intensity
modulated external radiation therapy), followed immediately in February 2009
with 5 sessions of Chemo using Taxotere, and in March 2009 with 12 months of
ADT using Trelstar (equivalent to Lupron for testosterone suppression). Since then, his PSA has been undetectable!
More
retrospective thoughts: He blindly
accepted his urologist’s recommendation for surgery, which was “conveniently”
available in two weeks. Although at
first it seemed the cancer was gone, he was surprised to find it returned. He feels now that radiation should have
promptly followed the surgery (common practice today, but not back then). He did become his own case manager, found the
IPCSG, and went to a prostate cancer specialist (late 2008). Together with this doctor, his best course of
action was mapped out: radiation, chemo, and ADT. He researched the best doctors for the
subsequent treatments (three doctors for each, always asking “if you had my
problem, who would you go to?”), and is alive and healthy today.
Recommendations: “Be your own case manager!” Seek out the best doctors, and don’t be
afraid to FIRE YOUR DOCTOR – John has fired three. Request and keep copies of all your medical
records. Carry a condensed medical
history, including a) Current medications, dosage, date started and
doctor. b) Discontinued medications c)
Over-the-counter supplements (including list of ingredients) c) Any allergies.
d) List of surgeries and procedures, dates, where performed, and doctor. e) List
of your doctors with address and phone. f) Your pharmacy with address and
phone.
Parting
thoughts, regarding “yesterday” vs. today:
He doesn’t put off routine medical appointments and checkups. He researches and understands his lab
reports. He asks the doctor
questions. He eats more moderately, and
reduces consumption of sugar, salt and alcohol.
He uses a respirator around chemicals and in the attic. He does still eat red meat and desserts. He enjoys every day, not being hyper-focused
on work. He takes vacations.
Questions:
Why
can’t we trust our doctor to give us good information – why do we need the
IPCSG to be able to get it right? It’s
the specialization and fast-changing developments; the ordinary doctor can’t
keep up. Seeing an oncologist (rather
than a urologist) is a help.
What
did Elliot mean by “3D MRI”? It’s the
current advanced MRI, such as is available at Imaging Healthcare Specialists
(more often referred to as mp-MRI, or 3T MRI, or nowadays, just “MRI.”)
More
details are given in the video of these presentations, including the PowerPoint
slides, which will be available for purchase via the website shortly before the
next meeting, or at the March meeting on the 16th.
-------------------------------------------------------------------------------------------------------------------------------------------------------------0
By Steven Reinberg HealthDay Reporter
TUESDAY,
March 5, 2019 (HealthDay News) -- Will an
aspirin a day keep prostate cancer at bay?
Not necessarily,
according to new research.
Danish
scientists say low-dose aspirin doesn't seem to reduce a man's risk of death
from prostate cancer, but it may slow down the disease in some cases.
For
patients with slow-growing, non-aggressive cancer, aspirin did appear to stop
the cancer from progressing. A slight benefit was also seen among men who took
aspirin for more than five years, the researchers found.
"Aspirin
is widely used due to its established protection against cardiovascular
diseases," said lead researcher Charlotte Skriver, from the Danish Cancer
Society Research Center in Copenhagen. "Our results, however, do not
suggest an overall protective effect of low-dose aspirin used in the year after
prostate cancer diagnosis on mortality from prostate cancer."
But
growing evidence suggests aspirin might reduce the risk of developing and dying
from colon and other cancers, Skriver said. It was thought that prostate cancer
could be added to that list.
Researchers
did see a small reduction in prostate cancer deaths among patients who took
low-dose aspirin for an extended time, she said. More study is needed to
confirm that finding.
Skriver
said any potential benefit from low-dose aspirin needs to be weighed against
the risk of gastrointestinal bleeding linked with its use.
For
the study, her team collected data on more than 29,000 men, average age 70, who
were diagnosed with prostate cancer between 2000 and 2011.
During
nearly five years of follow-up, more than 7,600 men died of prostate cancer and
more than 5,500 died from other causes, the study found.
The
findings were published March 4 in the Annals of Internal Medicine.
Dr.
Teemu Murtola, a professor of surgery at the University of Tampere in Finland,
wrote an editorial that accompanied the study.
"Aspirin
may have other benefits, but it is probably not helpful against prostate
cancer," he said.
Murtola
noted that aspirin was not associated in this large study with a lower risk of
death from prostate cancer, despite promising previous laboratory studies.
Still,
the risk was reduced among aspirin users in a subgroup of men with lowest-risk
prostate cancer, he said.
"Future
studies should aim to evaluate effects of very long-term, at least 10 years, of
aspirin use on risk of prostate cancer death," Murtola said.
Dr.
Anthony D'Amico, a professor of radiation oncology at Harvard Medical School in
Boston, said the study doesn't take into account the treatment patients
received -- an important point, because treatment directly affects survival.
Variables
such as surgery, radiation and hormone treatment are essential to tease out the
real effect of aspirin on survival, he said.
It's
not only the treatments themselves, but the combinations used and the duration
that can make a difference, D'Amico said.
"This
is not definitive, because there is too much lacking in terms of treatment
specifics," he said. "It's interesting, but it doesn't mean you
should take an aspirin."
More
information
The
American Cancer Society has more about prostate cancer.
SOURCES:
Charlotte Skriver, M.Sc., Danish Cancer Society Research Center, Copenhagen;
Teemu Murtola, M.D., Ph.D., professor, surgery, University of Tampere, Finland;
Anthony D'Amico, M.D., Ph.D., professor, radiation oncology, Harvard Medical
School, Boston; Annals of Internal Medicine, March 4, 2019
Last
Updated: Mar 5, 2019
Copyright © 2019 HealthDay. All
rights reserved.
https://www.onclive.com/web-exclusives/personalized-medicine-is-next-step-in-castrationresistant-prostate-cancer
Brandon Scalea
Raoul S. Concepcion, MD, FACS
The field of
castration-resistant prostate cancer (CRPC) is moving forward with the
development of several new treatment options, and the next steps for clinicians
will be tailoring treatment strategies to each individual patient, said Raoul
S. Concepcion, MD, FACS.
The phase III ARAMIS
trial introduced a third androgen receptor inhibitor that may shake up the
treatment paradigm for patients with nonmetastatic CRPC. In this study, the
addition of darolutamide to androgen deprivation therapy (ADT) was found to
significantly improve metastasis-free survival (MFS) versus ADT alone, with
comparable tolerability to enzalutamide (Xtandi) and apalutamide (Erleada).
The findings, which
were presented at the 2019 Genitourinary Cancers Symposium, showed the median
MFS was 40.4 months for patients treated with darolutamide compared with 18.4
months in those who received ADT alone (HR, 0.41; 95% CI, 0.34-0.50; P
<.0001). At a median follow-up of 17.9 months, the median time to pain
progression also favored darolutamide at 40.3 months compared with 25.4 months
with placebo, which translated to a 35% risk reduction (HR, 0.65; 95% CI,
0.53-0.79; P <.0001).
Although additional
data will be critical in determining where darolutamide will fit into the
nonmetastatic CRPC space, Concepcion, director of the Comprehensive Prostate
Center, and clinical associate professor of urology, Vanderbilt University
School of Medicine, said that cost could be the biggest deciding factor.
Beyond this approach,
immunotherapy in the form of PD-1/L1 inhibitors could soon have a more
significant role in the treatment of patients with metastatic disease,
Concepcion predicts. As the space continues to move away from traditional
approaches, the ability to interpret and utilize predictive biomarkers will
become all the more important, as they will help inform which treatment will
result in the greatest clinical benefit.
In an interview with
OncLive, Concepcion, who is also the editor-in-chief of Urologists in Cancer
Care, discussed the clinical implications of the findings from the ARAMIS trial
and highlighted other therapies that are coming down the pike for the treatment
of patients with CRPC.
OncLive:
How has the results from the ARAMIS trial impacted the nonmetastatic CRPC
landscape?
Concepcion: ARAMIS
was a highly anticipated trial mostly because the drug itself, darolutamide, is
structurally different than apalutamide and enzalutamide. In this trial,
investigators were looking at patients with nonmetastatic CRPC, a very similar
population to [those evaluated] in the SPARTAN and PROSPER trials. In other
words, these patients had a diagnosis of prostate cancer, were on ADT, had
testosterone levels in the castration range, and had rising prostate-specific
antigen (PSA). They were imaged and showed no evidence of metastatic disease by
traditional imaging, which includes a bone scan and a computerized tomography
scan. Enzalutamide and apalutamide are FDA approved for these patients. The
inclusion criteria for these patients was to have a PSA doubling time <10 a="" doubling="" has="" in="" less="" months.="" months="" patient="" population="" reality="" span="" this="" time="" when="">
The theory of
darolutamide being structurally different is that there may, in fact, be less
toxicity relative to central nervous system (CNS) adverse events. What they
reported out [at the 2019 Genitourinary Cancers Symposium] was what many people
anticipated: the time to metastases was delayed versus placebo. But what would
be the side effect profile? This [question] was specific to fatigue, because
enzalutamide and apalutamide have a very significant fatigue factor somewhere
in the order of 20% to 30%. What they reported at the symposium was that in the
darolutamide arm, the incidence of fatigue was approximately 15%; in the
placebo arm, it was 12%. Therefore, there is definitely a reduction in the
incidence of fatigue. Again, the delay to MFS was pretty much similar to what
we saw with enzalutamide and apalutamide in this nonmetastatic CRPC population.
These data are
significant, and there will be more data coming out on this. [The questions of]
how this is going to translate into practice and how we are going to use
darolutamide versus the other 2 agents still need to be flushed out. Cost will
be a big factor, and it will be interesting to see how long it will take for an
approval.
Where
do you see darolutamide fitting in this treatment paradigm?
This is going to be
an interesting question. Now, we have potentially 3 agents that have been
studied with positive trials in this setting. The challenge for clinicians is
going to be: which drug do we use? For urologists in particular, our experience
with enzalutamide going back to 2012 means that we are very comfortable with
using it. Because apalutamide has recently been approved [by the FDA] and it is
a very similar product, the urology world is getting used to this. With
darolutamide, once investigators start looking at the side effect profile, what
is going to be the willingness for the provider to use this drug? It will
probably be related to how they view individual patients. If you have a patient
who already has a lot of central nervous system toxicity and fatigue,
darolutamide may be a more preferable option. However, like anything else, when
you look at the primary endpoints, these drugs are very similar in their
results. It may ultimately just come down to cost.
What
is the importance of evaluating quality of life (QoL) in clinical trials?
We know there are so
many agents that prolong survival. What many people do not realize is that in
many of these patients with CRPC—especially if they are nonmetastatic—their
ECOG performance status is 0; they are highly functional and active. These are
not patients who are walking around in significant pain. The issue with some of
these agents is that their side effect profiles may set these patients back. If
therapy is going to slow down what patients are able to do on a daily basis,
that becomes significant. I'm glad we are emphasizing QoL into the equation
here. It is happening across the board with all of these targeted therapies,
and it should become the standard in clinical trials moving forward.
What
does the future hold for immunotherapy in prostate cancer?
Over the years, the
utilization of ipilimumab (Yervoy) had minimal efficacy in CRPC. However, we
know that mCRPC tumors are “cold” tumors—they are not that immunogenic. There
are a lot of data now, especially in men with mCRPC who have moved through
several lines of therapy, where we do see this mutational burden. There are
[biomarkers] that come as a result of treatment pressure selection. The 2 that
come to mind are microsatellite instability (MSI) and CDK12. If you take these
2 groups, a percentage of patients will actually respond to a PD-1/PD-L1
inhibitor. Therefore, there is going to be a place for our newer
immunotherapies, but what [this will depend on] is the clinicians understanding
which testing they need to order.
As we move from our
traditional therapies, the ability to interpret these predictive markers
becomes really important. Testing for MSI and CDK12 biallelic loss with
anticipation that we will also see [FDA] approvals for PARP
inhibitors—understanding where these factors lie, how to process the results,
and make them actionable is crucial. The challenge is going to be utilizing
these biomarkers and next-generation imaging.
What
are biggest challenges moving forward?
If we start from
initiation of disease, for newly diagnosed prostate cancer, the question is
going to be, “How can we determine who most needs treatment? Who needs active
surveillance?” Urologists are looking at that appropriately. We are even taking
that one step further in asking who we need to biopsy. Just because a patient's
PSA is elevated doesn't necessarily mean that they need to undergo a biopsy. We
are [working on developing] a better understanding of how to utilize PSA in
conjunction with some of this adjuvant testing—whether it be blood-based,
urine-based, or now, imaging-based with magnetic resonance imaging.
With definitive
therapy, some of the challenges are in patients with high-grade prostate cancer
who we know are going to progress. Who are the patients who will benefit from
adjuvant radiotherapy? We also know there are ongoing trials in patients who
have been definitively treated and have a biochemical recurrence. We know these
patients are at a higher risk of developing metastatic disease. The EMBARK
trial is looking at these patients and giving them ADT alone, enzalutamide
alone, or the 2 modalities combined; that will be a significant trial. Getting
back to localized prostate cancer, we know that there is a trial looking at
sipuleucel-T (Provenge) in patients who are candidates for active surveillance.
The point here is,
for the practicing urologists, to really look at prostate cancer and try to
isolate patients into these individual buckets. It does become a mastery of the
clinical trials and the particular phenotype we are dealing with, as well as
the drugs that are approved [by the FDA] or not. There is no doubt it is
becoming complex. We are going to see more agents, and we can guess that
immunotherapy will play a bigger role. We know some other mechanistic drugs
will come to the table. For urologists, it used to be operating, putting the
patient on ADT, then seeing what happens. Now, we have to critically look at
these patients.
Fizazi K, Shore ND,
Tammela T, et al. ARAMIS: efficacy and safety of darolutamide in nonmetastatic
castration-resistant prostate cancer (nmCRPC). J Clin Oncol. 2019;37(suppl 7S,
abstr 140). meetinglibrary.asco.org/record/170190/abstract.
------------------------------------------------------------------------------------------------------------------------------------------------------------
www.medscape.com
Roxanne
Nelson, RN, BSN
February
14, 2019
A
novel targeted radionuclide therapy has shown promising clinical activity and
low toxicity in a group of heavily pretreated men with metastatic castration-resistant
prostate cancer (mCRPC).
The
novel product is Lutetium-177 (177Lu)-PSMA-617 (under development by Endocyte)
is a radiolabeled small molecule that binds with high affinity to prostate
specific membrane antigen (PSMA), enabling tumor-targeted delivery of
beta-radiation. PSMA is over-expressed 100-1000 times in prostate cancers, and
expression is further increased in metastatic and castration-resistant
carcinomas.
The
new results come from an updated report on 50 patients with PSMA-positive mCRPC
who had progressed on standard therapies and were treated with the new product.
The results show a median overall survival of 13.3 months, which is longer than
the average 9-month survival time for men with this stage of disease, noted
lead author Michael Hofman, MBBS, a professor of nuclear medicine at the Peter
MacCallum Cancer Centre, Melbourne, Australia.
While
he believes that this may be a life-prolonging therapy, "this is not a
claim that we can make yet, because there's no comparator arm," he said.
Hofman
was speaking at a press briefing for this week's Genitourinary Cancers
Symposium (GUCS) 2019 in San Francisco, California. The study was presented
today at the conference.
"Metastatic
castration-resistant prostate cancer is a fatal disease and there is an urgent
need for new effective therapies," said Hofman, adding that based on the
results of this trial, two randomized trials were now underway.
One
is the TheraP trial, which compares LuPSMA with cabazitaxel (Jevtana,
sanofi-aventis) and the other is the VISION trial, which is comparing LuPSMA to
best standard of care; both trials are being conducted in men with
PSMA-positive, progressive mCRPC.
"This
is a very intriguing agent, and the VISION study is open in the US,"
commented briefing moderator Robert Dreicer, MD, of the University of Virginia
in Charlottesville and an American Society of Clinical Oncology
(ASCO)-designated expert.
"For
this group of patients in dire need of new options, using an entirely new
approach, this study provides hope that we can start to change their
outcomes," he added.
Prolonged
Survival, Decreased PSA
Hofman
noted that in an earlier study his team found favorable activity and low
toxicity in 30 patients with mCRPC. The current study is an updated report on
the safety and efficacy, and with a larger cohort and a median follow-up of
23.5 months.
In
this updated phase 2 study, the 50 patients received up to four cycles of
177Lu-PSMA-617 intravenously every 6 weeks. All patients had progressed on
standard therapies, and 90% of the men had been treated with abiraterone
(Zytiga, Janssen) or enzalutamide (Xtandi, Astellas) or both. The median PSA
was 190 and the median PSA doubling time was 2.6 months.
Eight
patients received fewer than 4 cycles owing to an exceptional response, Hofman
said, while 10 patients did not complete all planned cycles owing to disease
progression. The mean administered radioactivity was 7.5 GBq/cycle.
A
prostate-specific antigen (PSA) decline of ≥50% was achieved in 32 (64%) of 50
patients, including 22 patients (44%) who achieved a PSA decline ≥80%.
The
median overall survival was significantly longer among patients who achieved a
greater drop in their PSA levels: 18 months for those with a PSA decline of
≥50% vs 8.7 months for those with a decline <50 .001="" span="">
In
addition, 14 patients who progressed with PSMA-avid disease after the study was
completed received additional treatment with Lu-PSMA. In this patient subset,
64% had a PSA decline ≥50% and the median overall survival was 33 months.
The
most common toxicities associated with Lu-PSMA treatment were transient grade 1
to 2 dry mouth in 68%, grade 1 to 2 nausea in 48%, and grade 1 to 2 fatigue in
36%. Grade 3 to 4 toxicities were infrequent and included thrombocytopenia in
10% and anemia in 10% of patients.
The
study was sponsored by the Peter MacCallum Cancer Centre, Melbourne, Australia.
PSMA-617 was supplied by Endocyte and Lutetium-177 by ANSTO. Hofman disclosed
relevant relationships with Endocyte, Ipsen, and Sanofi. Coauthors disclosed
multiple relevant relationships with industry. Dreicer disclosed relationships
with Astellas Pharma, AstraZeneca, Genentech/Roche, EMD Serono, Incyte, Pfizer,
Seattle Genetics, Rainier Therapeutics, Janssen, and Merck.
Genitourinary
Cancer Symposium: Abstract 228. Presented February 14, 2019.
For
more from Medscape Oncology, join us on Twitter and Facebook
Medscape
Medical News © 2019 WebMD, LLC
Send
comments and news tips to news@medscape.net.
Cite
this article: Novel Radiotherapy Shows Promise in Heavily Pretreated mCRPC -
Medscape - Feb 14, 2019.
---------------------------------------------------------------------------------------------------------------------------------------------------------------
Posted
By Charlie Schmidt On February 25, 2019 @ 3:39 pm In Health,Living With
Prostate Cancer,Prostate Knowledge,Treatments | No Comments
Men
with advanced prostate cancer are typically treated with drugs that prevent the
body from making or using testosterone. A hormone (or an androgen, as it’s
known), testosterone drives prostate cancer cells to grow faster, so shutting
it down is essential to keeping the illness in check. About 600,000 men with
advanced prostate cancer in the United States today are undergoing this type of
anti-hormonal treatment, which is called androgen deprivation therapy (ADT).
But even as ADT helps men live longer, it exerts a toll on the body. Men can
lose muscle and bone mass, gain weight, and they face higher risks for heart
disease and type 2 diabetes.
The
good news is that a few helpful strategies can lessen these metabolic side
effects. Engaging in aerobic exercise and resistance training, for instance,
has been shown to drop levels of inflammation in the body that might otherwise
lead to heart disease. Quitting smoking is similarly beneficial, since tobacco
smoke’s toxic effects on the heart are more pronounced in the absence of
testosterone.
In
a new study, researchers have shown that taking daily walks and eating a
low-carbohydrate diet can also lessen ADT’s harms. During the investigation, 42
men who were just starting on ADT were split into two groups: Half the men took
daily walks lasting at least half an hour five days a week, and were instructed
to limit their carbohydrate intake to no more than 20 grams per day. The other
half of the men (the control group) maintained their usual diet and exercise
patterns.
After
six months, typical weight loss among men in the walking/low-carbohydrate group
was about 20 pounds, compared to a nearly 3-pound weight gain among men who
stuck to their usual dietary and exercise routines. Men in the
walking/low-carbohydrate group also had significantly higher blood levels of
high-density lipoprotein (HDL), which removes cholesterol and lessens risks of
atherosclerosis and heart disease. And they also had significant improvements
in insulin resistance (a pre-diabetic condition), but only at three months and
not when the levels were checked again three months later.
The
study’s lead author, Dr. Stephen Freedland from Cedars-Sinai Medical Center in
Los Angeles, California, says exercise combined with low-carbohydrate diets
appears to be a promising strategy in men undergoing ADT that should be studied
further. Dr. Marc Garnick, the Gorman Brothers Professor of Medicine at Harvard
Medical School and Beth Israel Deaconess Medical Center, and editor in chief of
HarvardProstateKnowledge.org, agreed, pointing out that weight gain can be a
real problem for men that endures even after ADT is discontinued. “The weight
loss in the experimental group is encouraging and should be validated in larger
studies,” he said. “In the meantime, combining exercise with low-carbohydrate
diets is a common-sense strategy that clinicians should recommend to their
patients.”
Article
printed from Harvard Health Blog: https://www.health.harvard.edu/blog
URL
to article:
https://www.health.harvard.edu/blog/diet-and-exercise-limit-heart-disease-risk-in-men-undergoing-hormonal-treatments-for-advanced-prostate-cancer-2019022516083
---------------------------------------------------------------------------------------------------------------------------------------------------------------
Date: February 28, 2019 Source: Sanford
Burnham Prebys Medical Discovery Institute
Summary:
Scientists have identified how prostate
cancer transforms into a deadly treatment-resistant prostate cancer subtype
called neuroendocrine prostate cancer (NEPC) following treatment with
anti-androgen therapy. Their findings -- which include the metabolic rewiring
and the epigenetic alteration that drives this switch -- reveal that an
FDA-approved drug holds potential as a NEPC treatment.
The
development of effective anti-androgen therapies for prostate cancer is a major
scientific advance. However, some men who receive these targeted treatments are
more likely to develop a deadly treatment-resistant prostate cancer subtype
called neuroendocrine prostate cancer (NEPC). No effective treatment for NEPC
exists.
Now,
scientists from Sanford Burnham Prebys Medical Discovery Institute (SBP) have
identified how prostate cancer transforms into aggressive NEPC following
treatment with anti-androgen therapy. Their findings -- which include the
metabolic rewiring and the epigenetic alteration that drives this switch --
reveal that an FDA-approved drug holds potential as a NEPC treatment. The
research also uncovers new therapeutic avenues that could prevent this
transformation from occurring. The study was published in Cancer Cell.
"Acquired
treatment resistance is a major concern for every oncologist. Eventually, over
enough time, cancer patients who receive a targeted therapy can become
resistant to treatment," says Darren Sigal, M.D., an oncologist at Scripps
Clinic and Scripps MD Anderson Cancer Center who worked with the scientists on
the study. "This study is an important advance that helps us understand
why targeted treatments for prostate cancer may promote the development of a
more aggressive tumor. These insights could lead to better treatments that help
fathers, sons and grandfathers around the world who are fighting prostate cancer."
Prostate
cancer is the second-leading cause of cancer death for American men, according
to the American Cancer Society. The cancer grows in response to hormones called
androgens. Targeted therapies that block these hormones have extended survival
for many patients. However, nearly all men eventually develop resistance to
these treatments. In 2019, more than 30,000 men in the U.S. are expected to die
from prostate cancer.
"Similar
to bacteria that gain resistance to antibiotics, tumors can become resistant to
anti-cancer drugs by 'remodeling' their environment and developing strategies
to evade targeted therapies. As targeted therapies become more potent, putting
more stress on tumors, we expect to see drug resistance become more
common," says Maria Diaz-Meco, Ph.D., the senior author of the paper and a
professor in the Cancer Metabolism and Signaling Networks Program at SBP.
"Our study shows that in a form of treatment-resistant prostate cancer, a
tumor suppressor gene called protein kinase C lambda/iota is downregulated. We
subsequently identified metabolic and epigenetic vulnerabilities which are
possible routes to prevent treatment resistance from arising."
In
the study, the scientists analyzed tissue samples from men with metastatic
NEPC, prostate cancer cell lines and a new mouse model of NEPC, created by the
researchers, to identify the molecular switch that triggers prostate cancer to
become treatment-resistant NEPC following targeted treatment. In addition to
detecting the downregulation of protein kinase C lambda/iota, the scientists
found that the NEPC cells upregulate the synthesis of a metabolite called
serine. Because serine is a non-essential
amino acid, treatments aimed at blocking
serine production may be devised that could impact the tumor with minimal or no
effect on the normal cells, thereby reducing potential toxicities.
Additionally, the researchers discovered that the cancer cells used a
communication pathway called mTORC1/ATF4 to accelerate the synthesis of serine,
allowing the tumor to grow faster and to epigenetically switch to the NEPC mode.
A protein that regulates the positions of lysosomes, the cell's degradation
machinery, was also involved in the tumor's transformation. Together, these
tumor characteristics represent novel approaches that could prevent prostate
cancer from transforming into NEPC.
A new identity
"NEPC
is essentially a new cancer. From what it 'eats' to how it looks, the tumor
cells are completely reprogrammed. The tumor even loses the receptor that is
targeted by current treatments, which is why it is so difficult to treat,"
says Jorge Moscat, Ph.D., a study author and director and professor in SBP's
Cancer Metabolism and Signaling Networks Program. "Identifying the switch
that drives the transformation from prostate cancer to NEPC is a critical first
step toward developing treatments that prevent treatment resistance in men with
prostate cancer before it begins."
The
scientists also identified epigenetic patterns -- molecular tags that modify
our DNA -- associated with NEPC, linked to the expression of an enzyme,
phosphoglycerate dehydrogenase (PHGDH), which could be a treatment target for
NEPC. Next, the scientists plan to work with SBP's drug discovery center, the
Conrad Prebys Center for Chemical Genomics (Prebys Center), to try to identify
a drug that can block PHGDH. The findings also indicated that an FDA-approved
drug that inhibits epigenetic changes, called decitabine, could hold promise as
a treatment for NEPC.
"Luckily,
prostate cancer is a cancer type that is well characterized, which helps us
better understand the mechanisms behind treatment resistance," says
Diaz-Meco. "With more research, one day we hope that no man dies of
prostate cancer."
Story Source:
Materials
provided by Sanford Burnham Prebys Medical Discovery Institute. Note: Content
may be edited for style and length.
Journal
Reference:
Miguel Reina-Campos, Juan F. Linares,
Angeles Duran, Thekla Cordes, Antoine L'Hermitte, Mehmet G. Badur, Munveer S.
Bhangoo, Phataraporn K. Thorson, Alicia Richards, Tarmo Rooslid, Dolores C.
Garcia-Olmo, Syongh Y. Nam-Cha, Antonio S. Salinas-Sanchez, Ken Eng, Himisha
Beltran, David A. Scott, Christian M. Metallo, Jorge Moscat, Maria T.
Diaz-Meco. Increased Serine and One-Carbon Pathway Metabolism by PKCλ/ι Deficiency
Promotes Neuroendocrine Prostate Cancer. Cancer Cell, 2019; DOI: 10.1016/j.ccell.2019.01.018
Cite
This Page:
MLA
APA
Chicago
Sanford
Burnham Prebys Medical Discovery Institute. "How prostate cancer becomes
treatment resistant." ScienceDaily. ScienceDaily, 28 February 2019.
.
-----------------------------------------------------------------------------------------------------------------------------------------------------------------
1.
How
prostate cancer becomes treatment resistant -- ScienceDaily: Scientists
have identified how prostate cancer transforms into a deadly
treatment-resistant prostate cancer subtype called neuroendocrine prostate
cancer (NEPC) following treatment with anti-androgen therapy. Their findings --
which include the metabolic rewiring and the epigenetic alteration that drives
this switch -- reveal that an FDA-approved drug holds potential as a NEPC
treatment.
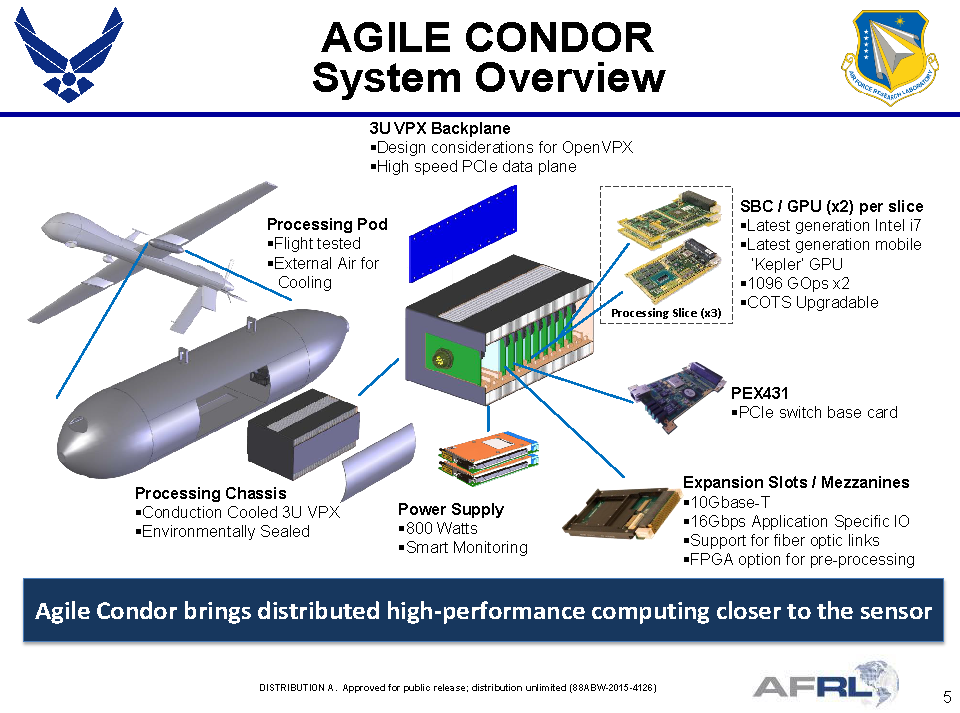
 Reaper Drones to Master AI with Agile Condor Super Computing Pod - Defense Update:: General Atomics Aeronautical Systems, Inc. has been awarded a contract from the U.S. Air Force (USAF) to demonstrate the Air Force Research Lab’s “Agile Condor” capability using a company-owned MQ-9 Remotely Piloted Aircraft (RPA). The testing will determine the optimum artificial intelligence and machine learning methodologies to find, identify and track select targets. Agile Condor also has the potential to dramatically reduce satellite bandwidth requirements as a result of its ability to automatically identify, classify, and nominate targets of interest. - Defense Update:
Reaper Drones to Master AI with Agile Condor Super Computing Pod - Defense Update:: General Atomics Aeronautical Systems, Inc. has been awarded a contract from the U.S. Air Force (USAF) to demonstrate the Air Force Research Lab’s “Agile Condor” capability using a company-owned MQ-9 Remotely Piloted Aircraft (RPA). The testing will determine the optimum artificial intelligence and machine learning methodologies to find, identify and track select targets. Agile Condor also has the potential to dramatically reduce satellite bandwidth requirements as a result of its ability to automatically identify, classify, and nominate targets of interest. - Defense Update: